Menopause and Hair Loss

What is Menopause?
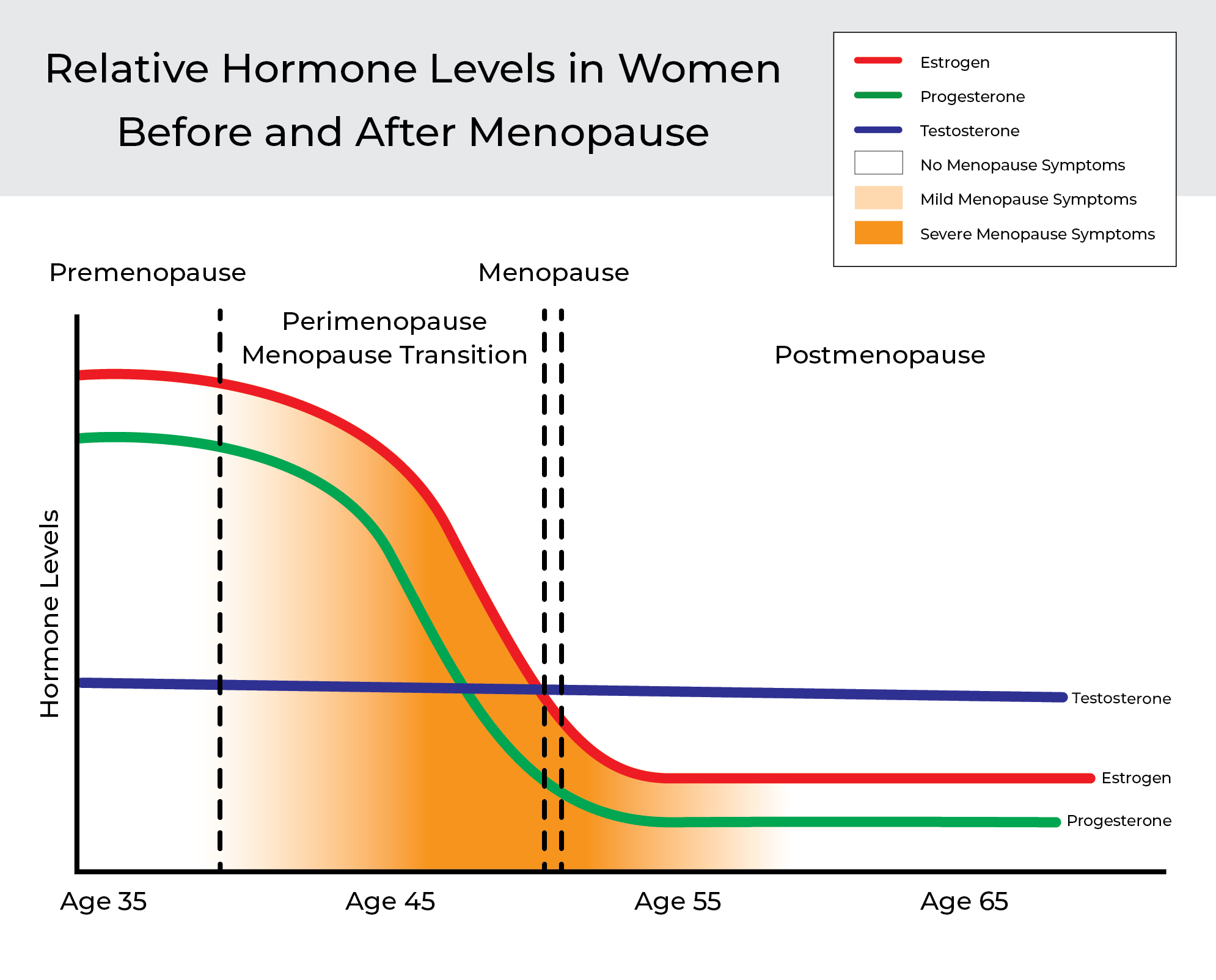
Menopause, unfortunately, is a normal and yet unavoidable part of ageing. As a woman ages, her reproductive cycles started since puberty slow down and prepare to stop. It happens when the ovaries no longer produce eggs and fewer female hormones: estrogen and progesterone levels reduce remarkably while the level of the principal androgen: testosterone, remains more or less the same or only slightly reduced. Both estrogen and progesterone control menstruation, but all three control hair growth in women together with other factors such as genetics, specific body regions and environmental influence.
Menopause is the stage in a woman's life when her monthly menstrual period stops permanently, thus marking the end of her reproductive years.
Natural menopause is the permanent ending of menstruation that is not the result of any medical treatment, surgery or medical condition and typically occurs in her late 40s to early 50s (45-55). However, some women can experience menopause earlier than 45, either due to body genetics, lifestyle, surgery (such as removal of the ovaries or/and uterus), or damage to the ovaries due to illness or medical treatments like radiotherapy or chemotherapy. Regardless of the cause, menopause occurring before the age of 45 is known as Early Menopause, with any occurrence by 40 or younger considered Premature Menopause.
Clinically Natural Menopause has Four Stages:
Although menopause is a well-known life stage in women, it is a gradual process with four different stages within menopause that are important to recognise and understand.
- Premenopause is the initial stage of menopause when a woman experiences NO signs or NO symptoms of perimenopause or menopause and still has periods (whether they are regular or irregular) and is still considered to be in her reproductive years.
- Perimenopause or "menopause transition" is the second phase/stage of menopause and is an ill-defined time that surrounds the final years of a woman's reproductive life. It begins with the first onset of menstrual irregularity or spotting and can start ten years before actual menopause. In some women, it can occur as young as 35 with an average length of about five years.
- Menopause is the point at which a woman no longer menstruates and has not done so for at least an entire year, i.e. 12 consecutive months after the final menstrual period.
- Postmenopause is the stage after menopause.
Genetics and Hair Loss
There's a lot of evidence pointing to genetics role in how you'll be affected and to what extent by perimenopause and menopause symptoms. In the absence of other influencing conditions like smoking, insulin intolerance, obesity and chemotherapy, it's most likely that your symptoms will mirror what your mother experienced. That's kind of like having a crystal ball into your future self's scalp hair, thus providing you with an opportunity to take precautionary action to get ahead of it! The earlier, the better!
Hair thinning and loss goes hand in hand with ageing and starts way before perimenopause and menopause. Many statistical studies into the prevalence of scalp hair thinning or loss in women in the western world came to very similar results/figures:
We're each born with around 102,000 hair follicles, and that's all we get! Your hair grows, regresses, rests, and sheds throughout your life in what's called the hair growth cycle. As we age, so does our hair resulting in a slowing down and shortening of your hair's growing phase.
In midlife/the mid-'30s, women experience physiological, emotional and physical changes to their bodies as their female hormones drop due to their in-coming menopause. The most substantial symptoms of menopause happen during the most significant drop in hormone levels.
According to most medical practitioners, one of the least concerning symptoms is scalp hair thinning and loss, but it can be a significant concern for all affected women and an understandably distressing experience for a woman of any age since, in many ways, hair defines a woman's identity. The resulting stress, if not resolved, or/and without proper counselling, support and assurance from the practitioner involved, unfortunately, will compound with the other common menopause symptoms like anxiety and depression, often making any hair loss situation even worse.
Negative changes in hair texture, thickness and growth result in scalp hair thinning or loss. Female Pattern Hair Loss FPHL is the most common form of alopecia (hair loss) in women. There are two ages of onset for FPHL: early (post-puberty to the third decade) and late-age (40+ years). Late-age onset is one of the most common symptoms experienced by women in premature menopause, the menopause transition (perimenopause) and menopause. The progressive shortening of the duration of hair in the 'growth' phase over successive hair cycles and the corresponding progressive follicular miniaturisation, i.e. the conversion from terminal hair to vellus hair* until the affected hairs eventually become invisible to naked eyes resulting in a reduction in the numbers of hair, especially in the central, mid frontal and upper parietal scalp regions with a characteristic pattern of hair loss starting as a widening of midline to a "Christmas tree" pattern. Refer to photos. Apart from FPHL, Telogen Effluvium (TE) is the 2nd most common scalp hair thinning or loss in females.

Figure Female hair pattern grading scale. Stages 1–5^.
Hormones and Your Hair - the Good and the Bad
Apart from genetic makeup, your hair thickness in shaft diameter and volume, growth rate, texture and condition are affected by many factors like hormones and nutrition, which play a very significant part in the quality and quantity of your hair. However, not all hormones are good for hair growth. The female hormones: Estrogen and Progesterone are good ones for hair growth, and androgens: testosterone (T) and its much more potent metabolite** dihydrotestosterone DHT (10 times more potent than T) are 'bad' ones well known for their key role in hair growth inhibition in a male's scalp hair loss, Male Androgenetic Hair Loss /Alopecia or simply Androgenetic Alopecia (AGA). However, in females, it is more complex than that as it involves androgen components and non-androgen components and other factors meaning that Female Pattern Hair Loss (FPHL) is the preferred and proper term rather than Female Androgenetic Hair Loss / Alopecia.
If you've ever been pregnant, you may have experienced the magic that extraordinary high levels of female hormones estrogens and progesterone bestow upon your hair during this time.
Estrogens are hormones naturally produced in the female body and consist of three major forms: E1 (Estrone), E2 (Estradiol) and E3 (Estriol). Estrogens can significantly promote hair follicle growth and prolong the hair growth cycle after binding to the locally expressed high-affinity estrogen receptors. Another protective action of Estrogens on hair growth is related to its negative influence on androgen metabolism/synthesis via the aromatase enzymes activity, which is responsible for converting androgens like testosterone and DHT to Estrogens instead thus, local androgen levels like DHT in the hair follicle is reduced along with its hair growth inhibition.
Progesterone can influence hair follicle growth through central and local action. Central action is referred to as the inhibitory effect on LH (Luteinizing hormone) secretion, which causes a decrease in ovarian theca cell stimulation (androgen synthesis). At the hair follicle level, progesterone decreases the conversion of testosterone to dihydrotestosterone (through the inhibition of 5-alpha reductase activity) and opposes its hair growth inhibition action.
It is widely known that Androgens such as testosterone (T); and dihydrotestosterone (DHT); and their prohormones, dehydroepiandrosterone sulphate (DHEAS) and androstenedione (A) - are the key hair growth inhibitors and determining factors in stopping scalp terminal hair growth. However, during pregnancy, they are counteracted by the hair growth-promoting effect of estrogens and progesterone.
The Androgen Paradox
Androgens stimulate beard growth but suppress scalp hair growth — this is known as the Androgen Paradox.
It is timely to mention that Mother Nature is so mysterious and wonderful that everything is not absolute. DHT, this potent androgen, is not always a 'bad' hair growth-inhibiting hormone. It also depends on genetics, specific body regions, timing and environmental influences, as mentioned earlier. DHT, the 'bad' scalp hair growth hormone on the scalp, becomes a 'good' hair growth-promoting hormone for other body parts except for the scalp, especially the face and the neck. Especially during a women's perimenopause, menopause and postmenopausal years, when it can cause undesirable excessive hair growth known as hirsutism with male characteristics and locations, making it a 'good' hair growth for non-scalp areas a 'bad' one for women.
Nevertheless, all hormones are the same: for hormones to work, function and exert their biological effects, they have to bind successfully to their specific receptors in the cells of target tissue — the hair follicle, per our current discussion).
Unfortunately, after childbirth, the benefits of those 'good hair pregnancy hormones' are lost while the 'bad hair hormones (T, DHT, prolactin, luteinising hormones LH, Cortisol the stress hormone etc.) become more dominant/influential, often resulting in short-term hair shedding and loss (postpartum hair loss).
Beginning in the third decade of life, cortisol levels in women and men increase gradually with age. Therefore, as we age, our cortisol levels rise. Cortisol is the stress hormone that controls and prepares our bodies, mood, motivation and fear to cope with any imminent crisis or threat to survival. Since Mother Nature will always choose survival above growth (including cell multiplication and reproduction), Cortisol also becomes a 'bad' hair hormone for hair growth.
During menopausal years: Declining estrogens and progesterone levels reduce their hair growth protective effect, combined with an increase or prolonged increase in cortisol levels, while your testosterone and DHT levels remain more or less the same, causes a reduction in the amount of time your hair spends in the growing phase of the hair growth cycle resulting in increased hair fall, thinning and loss.
Unlike postpartum hair loss, hair lost during perimenopause and menopause is often long-lasting, resulting in FPHL (Female Pattern Hair Loss), diffuse hair loss, chronic Telogen effluvium or even senescent alopecia/hair loss.
Can Hair Loss from Menopause be Minimised or Reversed?
Yes - When we consider that various nutrient molecules consumed in a normal diet provide energy for all living cells in our bodies. Including energy for hair growth in follicular cells, or act as precursors/building blocks in steroid and sex hormone synthesis and vital cellular messengers for various cell functions to initiate direct impact/effect on structure, growth, and keeping hair and skin integument.
We now know from decades of research that several vitamins and nutrient molecules positively influence and promote hair growth and overall hair and scalp health. Activance has taken this knowledge and utilised recent advancements in science and technology to create a range of cutting-edge, scientifically proven natural products with bioidentical*** and regenerative hair growth nutrient molecule Rhodanide.
Because Rhodanide, also known as Thiocyanate, is the vital nutrient molecule that our bodies produce naturally to keep our hair growing healthy and strong, any deficiency will reduce hair aesthetics and scalp health, accelerating hair damage, ageing and eventually thinning and loss. Unfortunately, our hair's Rhodanide levels are being constantly depleted by our modern-day lifestyle: washing, styling, chemical treatments, medicine/drugs, stress and health conditions, ageing as well environmental conditions such as chlorine from pool water and UV damage from the sun.
Using Activance leave-in treatments along with their supporting gentle shampoos and conditioners will replenish and boost lost Rhodanide and other essential nutrients, supporting your hair during perimenopause and menopause. When incorporated into your daily wellness routine in your younger years, it will provide you with a lifetime of thick, beautiful, healthy hair.
The three powerhouse ingredients in Activance each essential for your hair and scalp health are:
- Rhodanide (Thiocyanate) — the principal bioactive ingredient in Activance is a natural, bioidentical, bioactive nutrient molecule vital for hair growth, health and quality. It plays an essential role in activating dormant cells, increasing metabolism, cell multiplication and growth. It is a natural androgen receptor blocker competing with DHT to engage with the androgen receptors, thus relieving/reducing the DHT hair growth inhibition of on scalp hair follicles. Please refer to Literature reference for details****. It is a safe and effective molecule that works in harmony with the body's biology, delivering hair and scalp health for all. In 2017 it was classified as "Generally Recognised As Safe (GRAS) food additive by FDA".
- Fructooligosaccharides (FOS's) and Beta Vulgaris (Beet) Root Extract. FOS'S is a natural prebiotic complex with proven vitamin D like activities. Apart from its well-known importance in bone health, maintaining our body's reserve of calcium and phosphorus, Vitamin D is vital for hair growth and healthy scalp/skin. FOS's complement and enhance the regenerative hair growth molecule Rhodanide while further improving hair aesthetic, moisturising the hair and scalp while supporting and normalising the beneficial microbiome's growth on the scalp epidermis.
- MSM (Dimethyl sulfone) is a naturally occurring sulphur compound so integral to life that it is present in the cells of every living plant and animal on earth. Donating the "sulphur" element as a building block to form various vital proteins and enzymes containing Sulphur amino acids like taurine, cysteine and methionine as precursors for making keratin hair protein. Therefore, maintaining a constant supply of MSM is fundamental to the healthy production and maintenance of our hair, skin, and nails. Apart from its great soothing action, working in synergy with Rhodanide, MSM dramatically increases hair moisture levels and blood circulation in the scalp, facilitates repairing damaged hair, and assists other nutrients resulting in thick, strong, shiny, and healthy hair.
Advice on Hair Loss from Menopause
The symptoms of perimenopause and menopause can be distressing for many women; through our head office, we can offer general advice on hair loss and thinning associated with this stage of your life over the phone.
Alternatively, you may wish to attend our Activance Clinic for a one-on-one personalised consultation with Regenerative Health Consultative Pharmacist Arthur Chan. Arthur has worked in regenerative health, specialising in ageing, immunity, hair and skin, and general wellness for over 20 years.
If you require assistance or have any questions regarding this blog, please feel free to contact us.
*Terminal hairs are thicker, longer and highly pigmented. In contrast, vellus hair is very fine, soft, short non-pigmented hair.
**The definition of a metabolite is "a substance formed in or necessary for metabolism".
***The medical definition of bioidentical is "having the same molecular structure as a substance produced in the body".
****Sodium thiocyanate: a probe for the conformations of the androgen-receptor complex.
Recent Posts
-

Discover The Truth On How Often We Should Shampoo Our Hair
And its effects on Hair Loss, Aging and Hair and Scalp Health. The Results are in from the Acti
-

Uniquely different but Equally Effective Hair Health & Growth Ranges
What's the difference between Activance Hair Wellness & Activance Professional? That's one of o
-

Is your shampoo the culprit for triggering hair loss?
Could the Wrong Shampoo be Causing Your Hair Loss Issues? Many people experience hair loss at s